
We Adapted the Duluth Power and Control Wheel for Insurance Companies and Therapists. Here's Why.
When a colleague we'll call Anna read the first words of the first wedge on the wheel we're about to show you, here's what she sent back:
"Just read the first few words of the first item, USING COERCION AND THREATS, and I got sort of sick and scared at the same time. Whoa."
That's the response we keep getting, not just "interesting," or a "good point," but a full body and nervous system response. The same kind of response that survivors of domestic abuse describe when they first see a Power and Control Wheel and recognize their own life on the page.
We made this wheel because, after over 20 years in private practice and coaching tens of thousands of therapists, we were running out of language for what we were watching happen to our colleagues. The word "burnout" kept getting thrown around like it was a personal problem, while the word "challenges" kept getting used by associations that should have known better, and "headwinds" is being used to describe what’s happening in insurance industry reports.
None of those words names what is actually happening.
What is happening is a coordinated pattern of behavior by insurance companies and venture-backed therapy platforms that, when you map it out wedge by wedge, looks alarmingly like the pattern that Ellen Pence, Coral McDonnell, and Michael Paymar mapped out in Duluth, Minnesota, in 1982, when they sat with battered women and asked them to describe what their partners were doing to them.
We are here, naming a pattern.
This is going to be a long read because that is what is needed to convey the message. If you are a therapist who has been on insurance panels in the last five years, or who has tried to leave one, or who has watched a friend cry over a clawback letter, we want you to find yourself somewhere in this piece and to feel less alone. We want you to know that the pattern you have been gaslit about, that keeps being called your fault, and that has eaten your evenings and your weekends and your savings account, is a real pattern with a real name.
That pattern is called power and control.
A Note on the Framework We're Borrowing, and Why
The Power and Control Wheel was developed in 1982 by Ellen Pence, Coral McDonnell, and Michael Paymar at the Domestic Abuse Intervention Project (DAIP) in Duluth, Minnesota. It was built out of focus groups with women who had been battered. The wheel was based on women’s testimony, not theory, as they were asked what should be taught in court-ordered groups for men who batter. They answered with the tactics, the daily mechanics, the way the threats and the kindness and the isolation and the money worked together to control them.
The wheel is, in DAIP's own words, "a conceptual tool" rather than a theory. It "helps people see the patterns in behavior and their significance." Over the last forty years, that tool has been translated into more than thirty languages and adapted into more than forty variations, including a Medical Power and Control Wheel, a Workplace Bullying Power-Control Wheel (Barnes 2012, Scott 2018, peer-reviewed in nursing journals), a Lesbian/Gay Power and Control Wheel, an Abuse in Later Life Wheel, and many cultural adaptations. The National Center on Domestic and Sexual Violence is the clearinghouse.
We are not the first to use this framework for institutional and structural harm, nor will we be the last. We credit DAIP at the bottom of every version of the wheel we produce, and we honor the women whose testimony built it.
We want to say this clearly: insurance executives are not abusive intimate partners. The harm done by a person who batters their intimate partner is not the same harm done by a company that denies a panic-disordered teenager her tenth session. The stakes, the intimacy, and the type of terror are different.
What we are looking at is the similarity in the pattern.
The Wheel
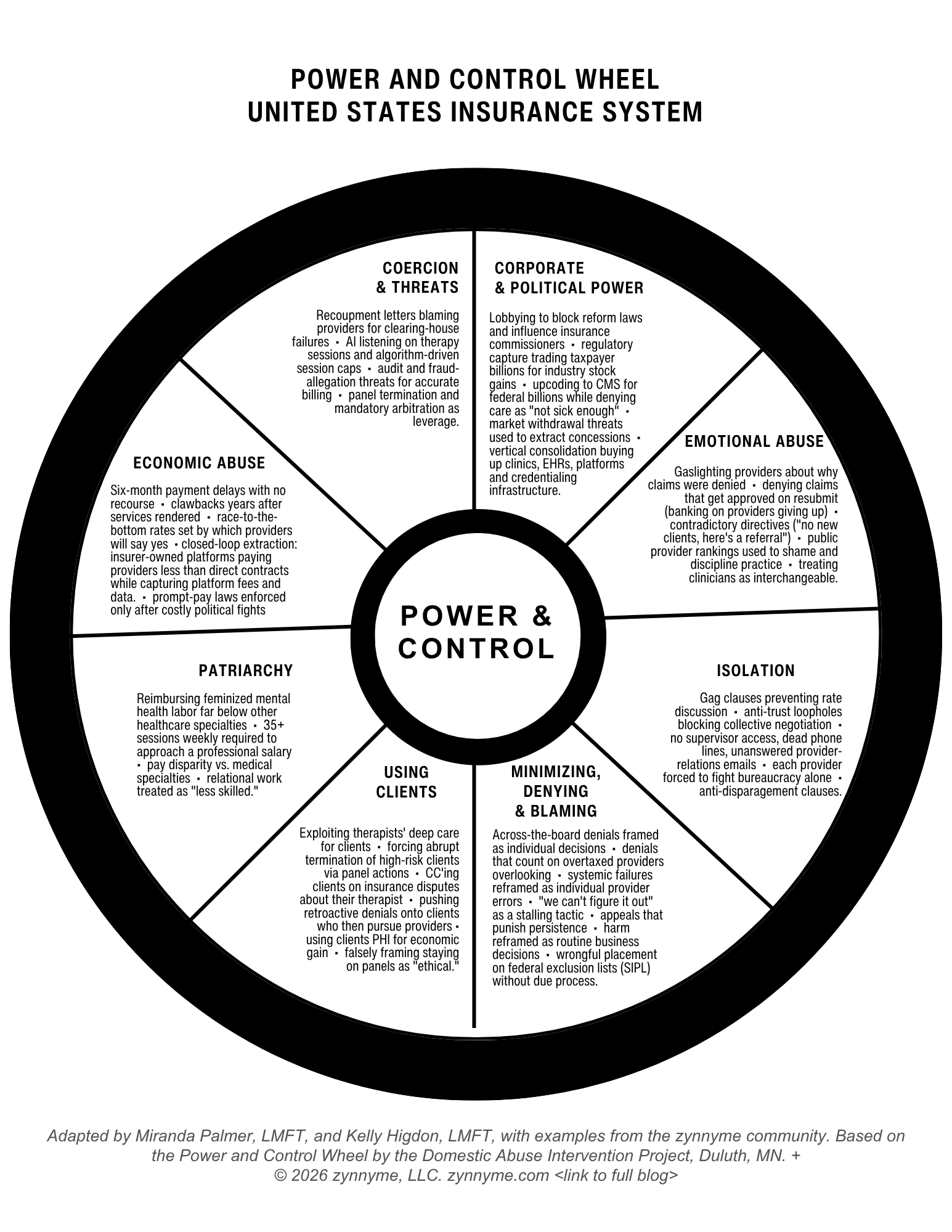
You will see eight wedges, each naming a category of tactic. The center says POWER AND CONTROL because that is what the tactics produce, working together, in coordinated fashion, over time. Each wedge below has its own story based on a real one from a therapist, told with pseudonyms and details altered for privacy. Each story sits next to documented industry examples.
Read them in order or jump around; they all connect.
Quick caveat: these are not exhaustive. We know you have your own stories. Below, you have an option to reach out to provide suggestions for updates, edits, or to include your stories.
1. Using Coercion and Threats
Recoupment letters blaming providers for clearing-house failures • AI listening on therapy sessions and algorithm-driven session caps • audit and fraud-allegation threats for accurate billing • panel termination and mandatory arbitration as leverage.
"BCBS didn't pay me for six months last year, and then sent me a very official letter closing my case, after six months, stating that it was my responsibility because I had filed under my social security number, which I had not. They owed me over 25k. I had to take it all the way to the Attorney General's office in Maryland to finally get a response." (Helen)
Coercion is when the system uses the fear of loss (your livelihood, your panels, your legal record) to extract compliance before any actual loss arrives. Each tactic below is engineered to make you cautious, quiet, and willing to absorb harm rather than push back.
Recoupment letters blaming providers for clearing-house failures. When clearing houses like Availity miss a step in the data handoff between insurers, the recoupment letters land in the provider's inbox, not in the corporate office that built the system. Helen received one for over twenty-five thousand dollars after six months of unpaid BCBS claims. The clearing house had pulled her SSN instead of her EIN. The original error was systemic; the cleanup was assigned to her, and the letter blaming her was CC'd to her client. She got the money back only after escalating to her state’s Attorney General. She is leaving BCBS, not because she could not survive it, but because she finally understood she was never supposed to.
AI listening on therapy sessions and algorithm-driven session caps. Platforms have begun inserting consent checkboxes for AI to listen to live sessions, transcribe them, and feed the data back into algorithms that flag therapists for caps, additional review, making clinical referrals, or rate adjustments. The therapist agrees in onboarding paperwork buried deep in the platform terms, and the client may or may not know. Platforms introduced this functionality in late 2025, before most therapists had a framework for what informed consent for AI session transcription even looks like. The session data, the diagnostic insight, and the relational labor are all extracted while the therapist's expertise is scraped into the model without compensation or any royalty payment.
Audit and fraud-allegation threats for accurate billing. Therapists report routine audits triggered by simple billing patterns (90837 over 90834, telehealth, weekly cadence) framed as fraud investigations. The audit becomes a punishment, and the absence of any actual finding is irrelevant to the chilling effect. The next time you bill that code, you hesitate, and that hesitation is the goal.
Panel termination and mandatory arbitration as leverage. Provider contracts increasingly include mandatory arbitration clauses, anti-disparagement clauses, and at-will termination provisions. The therapist signs a contract where the panel can drop them for any reason, the therapist cannot sue, and the therapist cannot publicly discuss what happened. The threat does not have to be used to work because the presence of the clause shapes behavior.
The pattern of coercion: extract compliance by threatening loss before the loss arrives.
2. Using Corporate and Political Power
Lobbying to block reform laws and influence insurance commissioners • regulatory capture trading taxpayer billions for industry stock gains • upcoding to CMS for federal billions while denying care as "not sick enough" • market withdrawal threats used to extract concessions • vertical consolidation buying up clinics, EHRs, platforms, and credentialing infrastructure.
"I love this Miranda. The rage I feel at the broken system, not just our mental health system, all of it, is just A LOT." (Devon)
The mechanics of corporate and political power are not abstract. They show up in specific legislative outcomes, specific regulatory rulings, and specific ownership structures.
Lobbying to block reform laws and influence insurance commissioners. Industry trade groups (AHIP, the Better Medicare Alliance, the Blue Cross Blue Shield Association) maintain a permanent lobbying presence in Washington and in every state capital. State insurance commissioners are frequently former industry executives, and frequently move back to the industry after their public-service stint. Reform bills routinely die in committee, while reform bills that pass routinely get watered down before signing. This is the normal operating mode of regulatory capture.
Regulatory capture trading taxpayer billions for industry stock gains. In May 2026, Congresswoman Alexandria Ocasio-Cortez questioned HHS Secretary Robert F. Kennedy Jr. about a $13 billion reimbursement increase the administration had just handed to Medicare Advantage insurers. CMS had originally proposed a near-flat 0.09% rate increase. Industry trade groups ran a pressure campaign, and Insurer stock prices dropped. Two weeks later, the rate increase was revised to 2.48%, and thirteen billion taxpayer dollars moved from the public to private insurers in fourteen days. Kennedy admitted on the record that insurers were lying, but the money flowed anyway.
Upcoding to CMS for federal billions while denying care as "not sick enough." By the federal government's own estimates, Medicare Advantage insurers defraud Medicare by approximately $80 billion per year by upcoding patients to claim they are sicker than they are, while simultaneously denying care to those same patients on the grounds that they are not sick enough. Both halves of the contradiction generate revenue and also harm the patient.
Market withdrawal threats used to extract concessions. When state legislatures or regulators consider rules insurers don't like, the industry threatens to withdraw from the market. Whole counties have lost their insurers when negotiations did not go the industry's way. The pattern is so reliable that regulators now anticipate it and pre-soften the rules before the threats arrive.
Vertical consolidation buying up clinics, EHRs, platforms, and credentialing infrastructure. Headway, the largest VC-backed therapy platform, took a $125 million Series C investment in 2023 that included Health Care Service Corporation, the Blue Cross Blue Shield licensee that serves more than 18 million members. UnitedHealth owns Optum, which employs or contracts with roughly one in ten U.S. physicians. And as of January 2026, the consolidation reached the upstream layer. CAQH, the nonprofit credentialing database that held 4.8 million provider records and sat upstream of nearly every insurance enrollment, directory listing, and claims process in the country, was formally acquired by a consortium of major health insurers. UnitedHealth, Centene, Cigna, Aetna, Elevance, Humana, and a coalition of Blue Cross Blue Shield plans now own it. The board chair is a UnitedHealth Group Executive Vice President. The vice chair is Centene's COO. In June 2026 they rebranded it DataSpring. The insurance companies that decide whether providers are paid, panels are open, and directories list us accurately now also own the system of record that holds market intelligence on every provider who competes with their VC-backed platforms. State regulators trying to enforce network adequacy laws now have to rely on a database owned by the entities they are regulating. The 120-day re-attestation cycle that providers must complete to stay listed is already being used as an enforcement lever; miss the window, and your directory listing, enrollment status, and claims processing can cascade into disruption.
Manufactured the problem, owns the solution. Insurance company directories are notoriously full of ghost networks: providers listed in the network who are no longer practicing, are not accepting new clients, or were never contracted with the insurer in the first place. One independent study found that more than two-thirds of networks examined had ghost provider rates over 9%. Clients call ten listed therapists and reach none.
The ghost network is the result of low rates that push therapists out, slow credentialing that traps therapists who want in, and directory data that the insurers have no operational incentive to clean. And then, with the ghost network problem fully manifest, the same insurance companies offer the solution: their own VC-backed platforms (Headway, Alma, Rula, Grow Therapy, BetterHelp), which have searchable, well-maintained provider lists and same-week availability. The problem the insurers manufactured creates the case for the platforms the insurers partially own.
Two federal bills (the REAL Health Providers Act for Medicare Advantage, signed into law, and the proposed Behavioral Health Network and Directory Improvement Act) attempt to address ghost networks. Illinois, Oklahoma, New Mexico, and Massachusetts have moved at the state level. As of 2026, federal enforcement is still being phased in.
Insurance company problem? Let’s create a law that impacts everyone BUT the insurance companies.
And then there is the bait-and-switch built into how reforms get implemented. The No Surprises Act, passed in 2021, is a useful case study. The original problem the law was meant to solve was hospital balance billing: patients getting hit with massive out-of-network bills after going to in-network hospitals where some specialists were not in-network. Patients complained, and Congress responded.
The Good Faith Estimate requirement that came out of that law landed first, and hardest, on a population that was not causing the problem: private-pay therapists, whose fees were already publicly transparent, whose clients were paying out of pocket by choice, and who were not part of the surprise-billing hospital ecosystem at all.
Therapists in private practice who did NOT take insurance were suddenly required to issue itemized twelve-month cost projections with CPT codes for every prospective client, maintain them in the medical record for six years, and provide patient dispute resolution language. Compliance deadline: January 2022. Of course, these good-faith estimates were required to be provided before ever seeing or assessing the client or having any knowledge of their needs, diagnosis, etc.
But, did the Good Faith Estimate actually fix the insurance company in-network hospital issue it was meant to fix?
The half of the law that requires insurance companies to provide advance explanation of benefits and good-faith estimates to insured patients has been delayed for five years and counting. The implementing agencies cite the complexity of insurance company systems as the reason. As of 2026, HHS has still not enforced this part of the law on insurers. The same agencies that gave therapists six months to comply with a five-hundred-page rule have given insurance companies five years to reach a deadline they may not actually have to meet. The pattern: patient complaints about insurer behavior produce regulation. The regulation gets implemented against providers immediately. The regulation against insurers gets postponed indefinitely. The insurance companies, who shaped the final rule, retain plausible deniability.
When private equity buys the clinics, the EHRs, the platforms, and the rate-setters, "competition" becomes a marketing term. When trade associations write the regulations and stock prices set the policy, "the market" is no longer setting anything. When upcoding for federal billions and denying care to actual sick people happen simultaneously, calling it a business model is too generous.
3. Using Emotional Abuse
Gaslighting providers about why claims were denied • denying claims that get approved on resubmit (banking on providers giving up) • contradictory directives ("no new clients, here's a referral") • public provider rankings used to shame and discipline practice • treating clinicians as interchangeable.
"There were several times that I received letters with someone else's name in the greeting. I had one provider services rep trying to tell me about her sister's illness and hospitalization. I received letters stating things that were patently untrue. Not only did I get burned out, but I almost decided to just forget about it and retire. I could identify in myself all the characteristics of fight, flight, and freeze (I did NOT get to fawn), and almost gave up completely." (Robin)
Robin did not give up, and she is leaving BCBS as soon as she can get things set up. Her body, however, was already keeping score. The mechanics of emotional abuse in this system are slower than the mechanics of economic harm, but they are not subtler.
Gaslighting providers about why claims were denied. You submit a claim, and it is denied with a reason that doesn't apply to the case. You appeal, it is approved, and the next claim is denied for a completely different reason. There is a Blue Cross Blue Shield company that has been blanket-denying every session for adjustment disorder after six months on the grounds that the DSM specifies a six-month limit on the diagnosis. That is not what the DSM says; instead, the DSM says the diagnosis is appropriate within six months of the stressor ending. The insurer's interpretation is clinically wrong, and it forces therapists to either spend hours on appeals they will sometimes lose, swap to a diagnosis that is not accurate to keep getting paid, or move clients through treatment before they are done.
Many therapists assume it is their mistake, so they sit with the shame. They wonder if they are bad at their jobs. In reality, they are simply being trained to doubt themselves. And here is the data point that confirms the gaslighting at the system level: in 2024, insurers reported zero behavioral health claims denied for "lack of medical necessity". Zero. That is not because medical-necessity denials stopped happening. It is because medical-necessity denials are the explicit parity-violation red flag, so insurers reclassify the same denials under "other reason not listed" instead. The harm continues, the category changes, and the reporting dashboards stay clean.
Denying claims that get approved on resubmit (banking on providers giving up). The single-resubmit approval pattern is so universal across panels that it has to be policy, not error. The math is simple from the insurer's side: deny everything once, pay only what comes back the second time, save the difference on the providers who never appealed. The providers who appeal are the ones who learn to spend their evenings doing it, and the providers who do not are the ones who eat the loss.
Contradictory directives ("no new clients, here's a referral"). "We have placed you on a hold for new clients. Here is a referral." "Your codes look wrong. We can't tell you which code is right." "You billed too much this quarter. The number we expect you to bill is confidential." These statements are designed to keep you off-balance so you spend your energy decoding instead of pushing back.
Public provider rankings used to shame and discipline practice. Insurer scorecards, "your peer cohort averages X" letters, algorithmic flags that show up next to your name in directories, performance metrics tied to vague benchmarks. Instead of helping you do better clinical work, these were designed to keep you trying to please an entity that has no investment in pleasing you back.
Treating clinicians as interchangeable. The deepest insult woven through all of this is the assumption that any therapist could be swapped for any other therapist. The client's specific relationship with you, the years of trust, and the attunement that took both of you to build, are invisible to the spreadsheet. You are a CPT code with a provider ID, and the reduction is its own form of abuse.
If you have cried in your car after a phone call with provider relations, that is your nervous system correctly identifying that something is wrong. Pay attention to it.
4. Using Isolation
Gag clauses preventing rate discussion • anti-trust loopholes blocking collective negotiation • no supervisor access, dead phone lines, unanswered provider-relations emails • each provider forced to fight bureaucracy alone • anti-disparagement clauses.
"This is so freaking accurate as that's exactly what I've been saying about during my months-long struggle with HealthNet. HealthNet refuses to allow me to speak with a supervisor, they are always 'in a meeting' no matter when I call, and they no longer have a phone number for provider relations, only an email that is never answered." (Sam)
Isolation in this system is structural, not metaphorical. Cutting off the channels through which a target could ask for help is one of the oldest tactics in coercive control. Insurance contracts have engineered this at scale.
Gag clauses preventing rate discussion. Most insurance contracts include non-disclosure or anti-disparagement clauses that legally forbid you from telling colleagues what you are paid. You sit in supervision with another therapist on the same panel, and you literally cannot ask each other what your reimbursement rate is. The rate variation across providers can be substantial, and the silence keeps everyone guessing.
Anti-trust loopholes blocking collective negotiation. Anti-trust laws prevent therapists from collectively bargaining for rates as independent contractors, while the same insurance companies operate as massive blocs and negotiate with the full weight of their corporate scale. This is the result of decades of industry lobbying.
No supervisor access, dead phone lines, unanswered provider-relations emails. When Sam tried to escalate her case at HealthNet, supervisors were "always in a meeting." The provider relations phone number had been retired, and the email address went unanswered. Meanwhile, HealthNet continued sending her new client referrals, even after telling her she was not allowed to take new clients. That is the system functioning exactly as designed: appear to comply with network adequacy requirements while denying access and payment to providers simultaneously, in different directions, with no accountable human in the loop.
Each provider forced to fight bureaucracy alone. The customer service script, the escalation path, and the lack of any human point of contact at the panels you depend on for your income are designed for this. The point is not to resolve your issue. It’s to exhaust you until you stop calling.
Anti-disparagement clauses. Many platforms and panels include non-solicitation clauses that forbid you from telling your own clients you are leaving. Anti-disparagement clauses forbid you from publicly discussing what happened to you. The threat of being sued for talking about your own experience keeps therapists silent in exactly the spaces where naming the pattern would protect each other.
The defense against isolation is community. It is colleagues who know what they are paid, what they are charged, and what they have refused. Insurance contracts are designed to prevent this.
5. Minimizing, Denying, and Blaming
Across-the-board denials framed as individual decisions • denials that count on overtaxed providers overlooking • systemic failures reframed as individual provider errors • "we can't figure it out" as a stalling tactic • appeals that punish persistence • harm reframed as routine business decisions • wrongful placement on federal exclusion lists (SIPL) without due process.
"I appreciate this view, Miranda. I have stories but choose not to re-traumatize myself. Suffice to say, your analysis is powerfully validating." (Jules)
Some stories are too heavy to retell. The fact that Jules has them, that she will not put them on the page, and that the wheel still validated something for her, is the whole point of this wedge. The reframing of harm is the move that makes everything else possible.
Across-the-board denials framed as individual decisions. When a Blue Cross plan blanket-denies adjustment disorder claims after six months, the company does not announce a policy change; instead, the company simply denies. Each provider's denial looks, on its own, like an individual case. The policy is invisible until enough providers compare notes. The pattern is the policy, and the policy is the denial. The denial is reframed as a clinical judgment that the company did not actually make.
Denials that count on overtaxed providers overlooking. In 2024, 19% of in-network claims and 37% of out-of-network claims submitted to Healthcare.gov plans were denied, per KFF analysis. Roughly one in five in-network claims. For 36% of all denials (over 28 million claims), the listed reason was simply "other reason not listed." And here is the part to sit with: less than 1% of denied claims are ever formally appealed. Of the appeals that do get filed, 40% to 75% are overturned. The math from the insurer's side is straightforward: deny everything once, pay only what comes back the second time, and pocket the difference on the providers who never appealed. The business model depends on the therapist being too exhausted, too rushed, or too uncertain to notice what was denied or to push back. Then the denials stop being an error and become revenue.
Systemic failures reframed as individual provider errors. Clearing-house glitches get blamed on providers. Platform errors get blamed on therapists who never touched the platform's code. Insurer-side data entry mistakes become "provider documentation issues." Helen's six-month BCBS nightmare was caused, in the end, by a coding error at Availity (the clearing house owned, by the way, by HCSC, the same Blue Cross licensee that holds a major investment in Headway) that pulled her SSN instead of her EIN. The system error became her professional record.
"We can't figure it out" as a stalling tactic. Three hours on hold becomes a documentation issue. The documentation produced becomes a different documentation issue. The new documentation reveals a coding question that turns into a peer review. The peer reviewer cannot be reached, so the case is escalated. The escalation is acknowledged but not resolved. Six months later, you are still calling, and the panel has had the use of your money the entire time.
Appeals that punish persistence. The forms are intentionally arcane while the portals time out. The required documentation changes mid-appeal, and the reviewer at the other end may or may not have a license. The "denial reason" may or may not match the actual policy. The appeal can take ninety days. By the time the answer comes, you have absorbed the loss, eaten the labor, and learned the lesson the system wanted you to teach: don't appeal next time.
Harm reframed as routine business decisions. Mass denials are "actuarial." Audit recoupments are "compliance." AI-driven session caps are "utilization management." Surprise bills to clients are "billing reconciliation." Every harm has a euphemism, and every euphemism is a tool. The euphemism is how the harm avoids accountability.
Wrongful placement on federal exclusion lists (SIPL) without due process. A licensed therapist in good standing was placed on the federal Suspended and Ineligible Provider List in 2025 by an insurance company that, when she pushed back, could not explain how she got there. The SIPL is a federal exclusion list maintained by CMS for providers who have had licenses suspended or have been investigated or convicted of fraud. None of those things had happened to her. CMS confirmed she was not on their list. The insurance company kept her flagged anyway. She had to terminate seriously mentally ill clients abruptly while she fought the listing. There is no formal due-process pathway for therapists wrongly placed on the SIPL by individual insurers; appealing requires escalation, hours, often legal help, and a willingness to keep showing up. The cost of the insurer's mistake is paid in clinical disruption and client harm before the insurer ever acknowledges the error.
This is the wedge that prevents the pattern from being named, and it’s also the wedge that this entire blog post is designed to dismantle.
6. Using Clients
Exploiting therapists' deep care for clients • forcing abrupt termination of high-risk clients via panel actions • CC'ing clients on insurance disputes about their therapist • pushing retroactive denials onto clients who then pursue providers • falsely framing staying on panels as "ethical."
"It feels so predatory… why are rates from Headway so much better with insurances than when we get individually paneled? Makes no sense. My goal is to grow and hire associates to expand my team. But I got a rate from Aetna for $70 (both intake and 60min session). Whereas Headway is paying me $120-130 for the same exact services. It's disgusting." (Viv)
We hold our clients close. That is the whole point. Healing happens in the relationship. Insurance companies and platforms know this as they have built a system that depends on it.
Exploiting therapists' deep care for clients. The way it works: you take Aetna directly for $70 a session. Aetna's group-practice contract requires multiple therapists before they will consider you. You are solo, so you go to Headway, where the rate for the same Aetna client is $120 to $130. You build a caseload through Headway. The platform makes the difference up, for now, because its insurer investors need the network. Then, when you have built your client base inside the platform, the rate gets cut. You cannot leave because you cannot take your clients with you. Notes and client lists do not export. The therapeutic relationship the client has with you is leveraged against you to keep you on a platform that no longer pays what it used to.
Forcing abrupt termination of high-risk clients via panel actions. When the insurance company places a therapist on a hold list, an exclusion list, or a directory removal, the immediate clinical consequence is that the therapist's most vulnerable clients lose continuity of care. The insurer is not making a clinical decision. The clinician is forced to do the clinical work of explaining, terminating, and finding referrals for clients who can least afford disruption. The cost of the insurer's mistake is borne by the people the insurer claims to serve. More broadly, the sickest patients get the most denials. Patients with more than 10 provider visits in a year experienced denied claims at a rate of 27% in 2024, compared to 14% for patients with fewer than three visits. The denial system targets the people who need care most. The therapist absorbs the clinical fallout. The system continues to advertise itself as if it serves patients.
CC'ing clients on insurance disputes about their therapist. BCBS sent Helen's client an enclosed letter regarding the dispute over Helen's six months of unpaid claims. The letter framed Helen as the source of the problem. The client was now in possession of an "official" statement about the therapist they were currently in treatment with. Just one of the many ways that integrating a third party into the therapeutic relationship can create confusion, triangulation, and distract from the real purpose of therapy.
Pushing retroactive denials onto clients who then pursue providers. Pat's personal insurance company re-reviewed her claims from three years ago and denied most of what they had originally paid. Her providers are now coming to her, the patient, for payment. She is being asked to fight an insurer she has no leverage with, even though she was not the one who submitted the bill. The labor of getting paid is being pushed onto patients and providers simultaneously, while the labor of denying payment is being centralized inside a single corporate office that suffers no consequence for any of it.
Falsely framing staying on panels as "ethical." Many insurance contracts and panel agreements lean on this without ever saying it directly. It's as if the ethical responsibility for keeping a panel relationship alive belongs to you, that to accept unsustainable rates is part of your fiduciary duty to clients, and as if the only path to caring for marginalized clients is staying on a contract that is making you sick. This is the trump card that has kept more therapists on panels than any other. Care is what brought us to this work, and it is what is being weaponized.
You can leave a panel and still love your clients. You can be a brilliant clinician and decline to bill insurance. You can build a sliding-scale private practice that serves marginalized clients better than your in-network practice ever did, because you are no longer drowning in the labor of fighting denials. Staying is not the ethical choice, but sometimes leaving is.
7. Using Patriarchy
Reimbursing feminized mental health labor far below other healthcare specialties • 35+ sessions weekly required to approach a professional salary • pay disparity vs. medical specialties • relational work treated as "less skilled."
"The patriarchy piece in your wheel is spot-on. Let's not forget that when we are in PP we are taxed at a higher tax rate, at least in Maryland. No benefits, leave, vacation, employer contributions to retirement. Ugh." (Marcie)
Therapy is feminized work as the profession is approximately 70 to 80 percent women. The work itself is relational, emotional, attuned, and often called "soft skills" by people who have never done it. In our economy, feminized work is structurally underpaid. This is documented. The patriarchy wedge is the one that makes the others stick.
Reimbursing feminized mental health labor far below other healthcare specialties. When an insurance company reimburses a therapist $70 for an hour with a suicidal client, they are not making a market-driven decision. They are making a gendered one. They are betting that the therapist, mostly a woman, mostly a mother, mostly running on the fumes of vocational devotion, will say yes. They are right often enough that the system continues to function.
35+ sessions weekly required to approach a professional salary. Therapists in many states need to see 35 or more clients per week to clear what would be a beginning W-2 mid-career salary in another health profession. The number is a clinical impossibility for most therapists doing relational depth work while also running all aspects of a business. Sustaining presence with 35 humans per week, in 50-minute increments, while also handling documentation, billing, and the appeal cycles described in the rest of this wheel, is a recipe for catastrophic burnout. Many cannot do it for long. Many burn out and leave the field.
Pay disparity vs. medical specialties. The pay disparity between therapists and physicians for the same hour of patient care is not explained by training (a master's-level therapist may have more clinical hours of training than a psychiatrist), nor is it explained by demand (mental health is in a documented access crisis), nor is it explained by outcomes (therapy is one of the most effective evidence-based interventions in medicine). The disparity is explained by patriarchy. The largest U.S. health insurers continue to post record profits while therapists remain one of the lowest-paid master's-degree professions in the country. When we surveyed therapists about their monthly revenue, responses ranged from $547 to "Hahaha, I'm living paycheck to paycheck."
Relational work treated as "less skilled." The cultural framing of therapy as "talking" rather than as the highly trained synthesis of theory, clinical judgment, attunement, ethical decision-making, and somatic awareness that it actually is, is one of the foundations the underpayment rests on. If the work were valued accurately, the rates would not hold.
This wedge is also where the lack of benefits sits - no paid leave, vacation, employer contributions to retirement, paid maternity, and more. Instead, we are faced with self-employment tax that runs higher than W-2, and the lack of safety net for therapists in private practice mirrors the lack of a safety net for women workers across the U.S. economy. This is not because therapy is not valuable. This is because of who does the work.
8. Using Economic Abuse
Six-month payment delays with no recourse • clawbacks years after services rendered • race-to-the-bottom rates set by which providers will say yes • closed-loop extraction: insurer-owned platforms paying providers less than direct contracts while capturing platform fees and data • prompt-pay laws enforced only after costly political fights.
"I'm even getting clawbacks, if you call it that, where my personal insurance company re-reviewed claims paid 3 years ago and denied most of what they originally paid. Now my providers are coming to me for payment. How do you even fight these absurdities?" (Pat)
This is the wedge most therapists feel first and name last. The mechanics are familiar to anyone who has been on a panel for more than two years. It is a system designed to make sure the people doing the work cannot keep what they earn.
Six-month payment delays with no recourse. Payment delays of sixty, ninety, and even one hundred eighty days are routine. The provider absorbs the time value of the money. The insurer earns interest on the float. The arithmetic favors delay. The legal threshold for forcing payment is high. By the time you have a case, you have already paid the cost.
Clawbacks years after services rendered. Pat described one version of this from the patient's side. Her insurer re-reviewed claims paid three years ago and denied most of what they had originally paid. Her providers are now coming to her, the patient, for payment. She is being asked to fight an insurer she has no leverage with. From the provider side, clawbacks land without warning, sometimes for clients you no longer see, sometimes for codes that were approved at the time and re-categorized retroactively. The labor of denying payment is centralized. The labor of fighting the denial is dispersed across every provider it touches.
Race-to-the-bottom rates set by which providers will say yes. Reimbursement rates are not set by what the work costs or what the work is worth. They are set by what therapists, in aggregate, will accept. The desperate provider sets the rate, and the most exhausted provider sets the floor. The race goes downward.
Closed-loop extraction: insurer-owned platforms paying providers less than direct contracts while capturing platform fees and data. Headway, Alma, Grow Therapy, Rula, and BetterHelp are venture-backed entities with growth-and-exit timelines. Their financial logic is: pay therapists more than direct insurance early, capture market share, then squeeze the rate. What therapists in our community started naming through 2025 and into 2026 was that the growth model has a second floor. Several of these platforms are partially owned, through the VC arms of insurance companies, by the same payers therapists are otherwise contracting with directly. Headway has HCSC investment. Alma was backed by Optum Ventures and Cigna Ventures. Rula has investment from the Blue Venture Fund (a BCBS investment arm). A therapist we will call Tess named the dynamic precisely:
"So I recently contracted with Aetna in Utah and the rates were not only lower than Headway by about $40, when I pushed back on my credentialing service I was told 'that Aetna would need to see how I was serving their clients before they would consider an increase.' I don't think I am going to be taking Aetna clients for anything other than groups and have no problem telling clients why. I recently also saw a BCBS plan endorsing these 'partner' companies even though they will also reimburse telehealth with therapists of clients' choice outside of platforms. But it was all in the frame up. These larger companies are using these VC companies to not only funnel clients to themselves but are also effectively using the VCs to 'pay' themselves using 1099 labor." (Tess)
The insurer pays the platform at some rate per session. The platform is partially owned by insurer VC money, so the platform takes its cut. The therapist is the 1099 labor at the bottom. The amount the insurer pays through the platform can be substantially less than what they would pay a directly-contracted therapist (in Tess's case, forty dollars less per session in Utah). When she tried to negotiate the direct rate, Aetna told her she would need to prove herself with their clients first. The platform rate is the new floor, while the direct rate has been moved out of reach. Patient premiums flow in, value flows up to the platform (partially owned by other insurers), the therapist receives the leftover, and the data generated by the therapist's labor flows back upstream. Money in. Money up. Data up. And the therapist is at the bottom of the pyramid, doing the actual work.
Prompt-pay laws enforced only after costly political fights. Texas passed a prompt-pay statute with teeth after a years-long political fight that required millions of dollars and significant organizing. Where the laws exist, they exist because therapists and other providers spent years pushing for them. Where they do not, the cost of fighting for them sits on top of every other labor already extracted from the field.
This is what economic abuse looks like at scale: a system designed to ensure the people doing the work cannot keep what they earn.
The Pattern is the Point
If you read each wedge in isolation, you could call any one of them an unfortunate incident, a bad letter, a confused provider rep, a clearing-house glitch, a policy change, or just a bad week.
This is exactly the framing that has kept therapists from naming what is happening for fifteen years and more. Each incident is presented to the affected therapist as their own individual problem. The therapist absorbs the cost while they appeal and eat the lost income. The therapist wonders if they are not cut out for this anymore, questioning whether they should have used a different code, hired a different biller, or joined a different panel.
The wheel exists because the incidents are not individual, but instead they are coordinated. The same eight categories of behavior show up across every insurance company, every platform, every contract, and every state. The pattern is what makes this a system rather than a series of mistakes. The system is what makes the harm impossible to fight one denial at a time.
When you read all eight wedges together, you may notice your body doing things like tightening in the chest, heat rising in the face, the urge to throw your phone, and tears. Or you might have the opposite: a numb stillness, an "of course." Both responses are valid and are evidence.
If you have been carrying the shame of "I should have been better at the business side," put it down. There is no version of "better at the business side" that fixes a system designed to extract value from your labor.
If you have been carrying the rage of "this should not be legal," carry it. Some of it is not legal, and some of it is legal because the industry wrote the law. You are allowed to be furious about both.
If you have been carrying the exhaustion of "I just need to figure out how to make this work for one more year," we see you. We have been there. We have coached therapists through it. We have made our own decisions about it.
You are not the problem; this pattern of power and control is.
Safety Planning While You Are Still In It
In domestic violence work, "safety planning" is a specific intervention. It does not assume you can or will leave. It assumes that some people, for many reasons, are not in a position to leave today, and that the work in the meantime is to keep you as safe as possible inside a situation that is harming you.
We are using the same word deliberately. Many therapists are not in a position to walk off insurance panels tomorrow. Many have financial obligations to families or professional obligations to group practices, their employer, or contracts that they can’t exit this very moment. The point of safety planning is not to push you out but to help you stay sane.
A few things that have helped the therapists in our community.
Document everything. We mean document every denial and phone call, every confused letter, every promised callback that did not come, every CPT code rejection with date, time, name of the rep, and reference number. The act of documenting is a practice, and it is also psychological. It transfers the reality of what is happening from your nervous system, where it is being stored as your fault, to the paper, where it can be seen for what it is. We have had members come back months later and read their own documentation logs in disbelief, unable to deny what is happening.
Find other therapists who are seeing the same things. Isolation is the system's favorite wedge for a reason. The single most protective thing you can do is talk to colleagues, inside a peer consultation group, a private practice community, or any space where you can say "this happened to me" and hear "yes, me too." If your current professional spaces are not safe to say these things in, find new ones. Your state association may or may not be one of them. Your supervisor may or may not be one of them. Listen to your gut about who is safe.
Protect your mental health like you would protect a client's. You would not let a client in crisis skip sleep, skip meals, isolate, or stop their own therapy. Do not let yourself. The signs of fight, flight, freeze, and fawn are your body correctly identifying a threat. If your nervous system is dysregulated by an insurance phone call, that is information to take seriously.
Trust your instincts. When something feels like it’s not adding up, it usually does not add up. When a denial reason does not match the policy, it usually does not match the policy. When you "feel crazy" reading a letter, the letter is usually doing something. The pattern is designed to make you doubt yourself when you need to doubt the system instead. Your clinical and business instincts are still good.
Get help with the business side without internalizing the shame of needing it. Billing is a specialized skill, and so is reading platform contracts and insurance compliance. Asking for help with these is the same as a client asking for help with a panic disorder. Outsource the parts you can and get clear-eyed about what the labor is costing you.
Safety planning is the work of staying intact inside a situation that is trying to deplete you. There is no shame in it and no judgment from us.
Making a Plan to Leave
Some therapists are ready to leave panels.
Now that doesn’t mean they are ready to leave all of them, or even leave them right this moment, but they are ready to leave one panel or more as soon as they can.
If you are one of them, here is what we have seen work, in language as plain as we can make it. (If you are working through the specific question of leaving a VC-backed platform, we wrote a more detailed checklist for that exit plan here. What follows is the broader version that applies to platforms and panels both.)
Give yourself a real timeline. Most therapists who leave panels do it on a six-to-eighteen-month plan, not a six-week one. The plan is mostly financial. How long can you tolerate a slower phase while you transition? What is your runway? What is your floor? What income do you actually need (not the income you have been told you need)? Run the numbers without panic, as the numbers are usually less terrifying than the imagined numbers.
Build the private-pay capacity before you leave. Most private-pay therapists are full because they show up clearly and consistently in the places their clients are looking for them, with a clear, actionable marketing plan that includes SEO with a real website that has specific niche language. They are also getting out from behind their computers and fostering relationships, even just a few key referral relationships, making a huge difference in a practice. None of this is overnight, and none of it is dependent on luck. It is work, and it is learnable, and it is yours to keep when you build it.
Transition clients ethically, not the way insurance forces you to. The insurance version of "ethics" is staying on a panel that is making you sick out of fear of abandoning clients. The actual ethics of termination are different. They involve adequate notice, careful coordination, real referrals, and honest conversations. We are taught to fear abandoning clients, but that would mean not doing any of those things. Most clients can hear "I am moving off insurance, here is what your options are, here is who I can refer you to" with more dignity than the system gives them credit for. Some clients will follow you to private pay, and some will not. Neither outcome is a failure of care.
Build multiple referral streams, not multiple income streams. "Passive income" gets sold to therapists constantly, and most of that advice ends up making you work harder for less money. Here is what is actually true: there are more people looking for therapy in this country right now than there are therapists available to see them.
Mental health professionals have largely been trained by schools and by panels and by professional culture to undervalue their own work. The therapists we know who feel free built multiple referral streams, so they were never dependent on a single source for the next client. Some of those streams are human: primary care doctors, school counselors, body workers, attorneys, community organizers, and other therapists in different specialties. Some are online: showing up clearly enough that you land on page one of Google for the people in your area looking for what you do, and that the AI tools the public is now using to find therapists are referring clients to you instead of trying to replace you with a chatbot. That is different from building multiple businesses on top of a clinical caseload. Most therapists do not have the bandwidth for the latter, and the people who keep selling that promise are usually selling you something.
Find your community early, and choose it deliberately. Leaving panels alone is much harder than leaving alongside other therapists who have already done it. You do not have to figure it out by yourself, nor should you have to.
And be intentional about who you spend that time with so you can be around therapists who have the same goals you have and the kind of energy you want to have in your own life. If the people in your current professional circles are mostly stuck in feeling trapped, victimized, and waiting for someone outside to save them, and if they do not live the kind of life you want for yourself (friends, connection, wellness, joy), they are not the people to look to for guidance in building that. Validation is not the same as community. We need both: we need to name what the system is doing to us, and we need to be around people who, alongside that naming, are still moving toward a life that is bigger than the system.
If any of this sounds like a sales pitch, we want to be very clear: leaving panels is not the only valid path. Some therapists stay on panels and work for systemic change. Some therapists work in community mental health and never go private. Some therapists work for VA or non-profits and serve populations that need them. There is no one right answer.
But if you have been told, by anyone, that staying on panels is the ethical choice, that taking insurance is the only way to serve marginalized clients, that going private-pay is selling out, please know: those framings benefit the insurance industry, and they are part of the wheel.
Advocating for Systemic Change
The wheel is also a map for where to push.
Report. Every state has a department of insurance, an attorney general's office, and (often) a department of managed health care that takes complaints, and they sometimes do something with them. Helen got her money from BCBS only after escalating to the Maryland Attorney General. The Texas Department of Insurance has prompt-pay enforcement powers because therapists and other providers spent years documenting and complaining. Your individual complaint may not feel like much. In aggregate, they are how policy moves.
Here is where to actually file. For state-regulated insurance issues: your state insurance commissioner (NAIC maintains the full list) and your state attorney general. California's Department of Managed Health Care has independent enforcement authority that goes further than the standard insurance commissioner in most states, and other states are beginning to adopt similar models. For ERISA-covered employer health plans: the U.S. Department of Labor's Employee Benefits Security Administration. For federal mental health parity violations: HHS and the DOL jointly oversee parity, with HHS handling individual market plans and DOL handling employer-sponsored plans. For Medicare or Medicaid issues: CMS. State licensing boards for therapists generally do not handle insurance complaints, but they may engage when clinical harm to clients can be documented as a downstream consequence of an insurer's action.
Document the pattern publicly. TikTok, Substack, your own blog, podcasts, panels at conferences, the pattern is invisible when each therapist keeps their story to themselves. The pattern is undeniable when hundreds of therapists post the same story with the same dates and the same denial reasons, and the same insurance companies. Trade journals and journalists are starting to pick this up. Becker's Payer has been covering insurance fines and the UnitedHealth criminal probe extensively. The Psychotherapy Action Network (PSIAN) is publishing research on Corporate Practice Management Companies. The pieces are out there, and we need more of them, with names and dates.
Use the tools that already exist. Therapists are not on their own when fighting denials. Several free or low-cost tools have been built specifically for this. ProPublica's Claim File Helper generates a letter requesting the insurer's full claim file, the internal document that often reveals what actually happened with the claim and why. Counterforce Health and FightHealthInsurance.com are newer tools that use AI to analyze a denial letter and draft an appeal letter for you. Less than 1% of denied claims are appealed nationwide. Forty to seventy-five percent of appeals are overturned. The bottleneck is not the strength of the appeal. The bottleneck is the labor of producing one, and these tools have substantially reduced that labor. Encourage your clients to use them. Use them yourself.
Support the political fight. Mental health parity is the law, has been since 2008, and is routinely ignored. The federal No Surprises Act was written to protect patients from emergency-room balance billing and is being applied to private-pay therapists in ways that the original drafters never intended. Reform requires legislators who understand the system. Reform requires lobbying counter-pressure to the AHIPs and Better Medicare Alliances of the world. Reform sometimes requires unionization-adjacent organizing, like California's AB 1340, which created a path for over 800,000 rideshare workers to bargain collectively while staying classified as independent contractors. The same model could be adapted for clinicians.
Join the organizations doing this work. PSIAN or The Coalition for Patient Centered Care State coalitions of independent therapists and some professional associations (not all) are pushing back on insurance practices. Find the ones in your state that are, pay your dues, and show up to meetings.
Refuse to do the work for free. Refuse to do free utilization-review calls. Refuse to absorb labor that the insurer is contractually required to do. Refuse to apologize for charging a fair rate. The cultural pressure on therapists to "be reasonable" about money is part of the patriarchy wedge. Reasonable, in this system, means cheap. You do not have to participate in that definition.
Tell other therapists. This wheel only does its work if people see it. Share it. Print it. Put it in your office. Use it in supervision. Use it in clinical training programs. Use it in your own conversations with colleagues when "burnout" comes up and you want to name what is actually happening.
You Are Not Alone
Here is what we want to leave you with.
If you saw yourself somewhere on the wheel, you are not making it up. The body response was real, and the recognition was real. The rage and the grief and the exhaustion are proportional and earned. You have been carrying a lot more than you should have had to carry.
If you have been called "burnt out" by a system that was burning you, the language was wrong. You were not burning out. You were being burned.
If you have wondered whether you are cut out for this profession, the profession is not the problem, and the people who choose to do this work are not the problem. The pattern is the problem.
We made this wheel because we were tired of not having a name for the pattern. We are sharing it because the pattern is bigger than any one therapist, any one panel, any one platform, and any one state. We are an industry of mostly women, mostly relationally devoted, mostly underpaid, in a country where private equity and venture capital have spent the last decade buying every entry point to mental healthcare. The conditions are designed to keep us isolated, ashamed, exhausted, and individually responsible for collective harm.
We do not have to accept those conditions, nor be silent about them. Nor do we have to do this alone.
If You Want Help Getting Out of This Relationship
We will not pretend this is easy or that there is a single path or that leaving is the only valid choice. Staying is not some moral failure either (some of you cannot leave, and the system has earned the blame for that, not you).
But if you want help thinking about any of it, we are here without judgment.
We have built a free training library for therapists working through these exact issues. Three of them are directly relevant to this wheel:
A training on VC-backed therapy platforms (Headway, Alma, Grow Therapy, Rula, BetterHelp): what their contracts actually say, how to read them, what it means for your practice if you sign one.
A training on navigating insurance panels: when it makes sense to stay, when it makes sense to leave, and how to do either with as little harm to you and your clients as possible.
A training on AI, ethics, and the fight to keep therapy human: what AI note-takers and session-listening platforms are actually doing with your client data, what informed consent for AI even looks like, and where the line is.
All of these are free.
Share this with the colleague who has been crying about a denial letter. Print it for your supervision group. Send it to the friend who is wondering if they need to leave the field. We made it for them and for you.
You are not alone, you never were, even though the system worked very hard to make you think you were.
Help Us Refine This. Share This. WriteAbout This.
This wheel and the analysis around it are a work in progress. The first version came from the community stories therapists sent us. We need more. If you have a story, a suggestion, a correction, or feedback that would make this sharper or more accurate, please email us at help@zynnyme.com. We are continuing to refine the wedges, and the next version will reflect what therapists tell us.
If you want to share the wheel or this post, please share it. Send it to your colleagues. Print it for your supervision group. Use it in trainings. Show it to your professional association. We want this to travel. The one ask: please keep the attribution on the wheel image intact when you share it. That credit is what keeps the framework honest as it spreads. Once this post is live, the image itself will carry a built-in link back to the full piece, so you do not need to add one separately.
If you want to adapt the wheel for a related context (a different healthcare specialty, a different country's system, a community organization's training program, a research paper, a conference presentation), please email us at help@zynnyme.com first. We are not trying to gatekeep. We are trying to keep the framework from getting repackaged with a few word swaps and a new author byline, which has happened to other adaptations of the Duluth wheel, and which makes the work weaker over time. We are happy to talk. We would love to know what you are doing with it and to connect therapists who are working on the same questions.
If you are a journalist, writer, or researcher interested in reporting on what is happening to therapists in the United States right now, please email us at help@zynnyme.com. We can point you to the documented industry examples, the academic literature, the regulatory record, and the political context. With their consent, we can also connect you to therapists in our community who have lived these stories and can speak on the record. Between us, we have practiced as licensed therapists since 2005 and 2008, and have been coaching therapists through this system since 2010. We have lived this from the inside, alongside the therapists we serve. We would love to help you tell the story well.
References:
On the Duluth Power and Control Wheel
Domestic Abuse Intervention Programs. "Social Change to End Violence Against Women." theduluthmodel.org. https://www.theduluthmodel.org/social-change-end-violence-women/
Domestic Abuse Intervention Programs. "The Development of the Power and Control Wheel." https://www.theduluthmodel.org/wp-content/uploads/2017/03/The-Development-of-the-Power-and-Control.pdf
National Center on Domestic and Sexual Violence. "Wheels Adapted from the Power and Control Wheel." https://www.ncdsv.org/publications_wheel.html
Scott, H.S. (2018). "Extending the Duluth Model to Workplace Bullying: A Modification and Adaptation of the Workplace Power-Control Wheel." Workplace Health & Safety, 66(9), 444-452. https://journals.sagepub.com/doi/full/10.1177/2165079917750934
On insurance and platform consolidation
Health Care Service Corporation. "HCSC Takes Lead In Strategic Investments Portion of Headway Funding Round." Oct 5, 2023. https://www.hcsc.com/newsroom/news-releases/2023/strategic-investment-headway-behavioral-health
Facundo, J. and Rucker, P. "UnitedHealth Has 2,694 Subsidiaries and Affiliates. Is It Too Big to Manage?" The American Prospect, July 16, 2025. https://prospect.org/2025/07/16/2025-07-16-unitedhealth-has-2694-subsidiaries-and-affiliates/
Becker's Payer. "150 Things to Know About the 'Big 6' Health Insurers." https://www.beckerspayer.com/payer/150-things-to-know-about-the-big-6-health-insurers/
Behavioral Health Business. "Small Providers Flock to Therapist Enablement Platforms at the Cost of Autonomy." May 27, 2026. https://bhbusiness.com/2026/05/27/small-providers-flock-to-therapist-enablement-platforms-at-the-cost-of-autonomy/
On the CAQH acquisition and DataSpring rebrand
Becker's Payer. "Major insurers take ownership of former nonprofit healthcare data organization." Jan 7, 2026. https://www.beckerspayer.com/m-and-a/major-insurers-take-ownership-of-former-nonprofit-healthcare-data-organization/
Becker's Payer. "Insurer-owned CAQH rebrands to DataSpring." June 2026. https://www.beckerspayer.com/leadership/insurer-owned-caqh-rebrands-to-dataspring/
On the AOC/Kennedy testimony and Medicare Advantage upcoding
Office of Rep. Alexandria Ocasio-Cortez. "Ocasio-Cortez Questions Secretary Kennedy on Decision to Send Billions to Insurance Companies. "https://ocasio-cortez.house.gov/media/press-releases/ocasio-cortez-questions-secretary-kennedy-decision-send-billions-insurance
On BCBS adjustment disorder denials and industry denial data
Griswold, B. "Blue Cross Denies Adjustment Disorder Claims After Six Months." Navigating the Insurance Maze. https://theinsurancemaze.com/bcdeniesadjustmentdisorders/
Griswold, B. "Which Health Plans Deny the Most Claims? Why Claims Are Denied, And What You Can Do About It." Navigating the Insurance Maze, March 2026. https://theinsurancemaze.com/which-health-plans-deny-the-most-claims-why-claims-are-denied-and-what-you-can-do-about-it/
Kaiser Family Foundation. "Claims Denials and Appeals in ACA Marketplace Plans in 2024. "https://www.kff.org/patient-consumer-protections/claims-denials-and-appeals-in-aca-marketplace-plans-in-2024/
On state enforcement, prompt-pay, and reporting agencies
Texas Department of Insurance. "Prompt Pay FAQ (SB 418). "https://www.tdi.texas.gov/hprovider/ppsb418faq.html
Becker's Payer. "13 Payers Recently Fined by States ."https://www.beckerspayer.com/legal/13-payers-recently-fined-by-states/
National Association of Insurance Commissioners. "State Insurance Departments." https://content.naic.org/state-insurance-departments
U.S. Department of Labor, Employee Benefits Security Administration. https://www.dol.gov/agencies/ebsa
On ghost networks and provider directory accuracy
Quest Analytics. "Ghost Networks in Healthcare: What They Are and How To Address Them." February 2026. https://questanalytics.com/news/what-are-ghost-networks/
Quest Analytics. "The REAL Health Providers Act Signed Into Law." https://questanalytics.com/news/requiring-enhanced-accurate-lists-of-health-providers-act/
On appeal tools for denied claims
ProPublica. "Claim File Helper." https://projects.propublica.org/claimfile/
Counterforce Health. https://www.counterforcehealth.org/
On mental health parity law and the No Surprises Act
U.S. Department of Labor. "Mental Health and Substance Use Disorder Parity." https://www.dol.gov/agencies/ebsa/laws-and-regulations/laws/mental-health-and-substance-use-disorder-parity
JD Supra. "No Surprises Act Implementation in 2026." https://www.jdsupra.com/legalnews/no-surprises-act-implementation-in-2026-4720339/
On organizing precedents for independent contractors
Office of the Governor of California. "Governor Newsom Signs Landmark Worker Legislation." Oct 3, 2025. https://www.gov.ca.gov/2025/10/03/governor-newsom-signs-landmark-worker-legislation-in-stark-contrast-to-trumps-assault-on-workers-and-government-shutdown
On Corporate Practice Management Companies
Psychotherapy Action Network (PSIAN). "New Research Reveals Therapist Concerns About Corporate Practice Management Companies (PMCs)." https://www.psian.org/blog/new-research-reveals-therapist-concerns-about-corporate-practice-management-companies-pmcs
All quotes from therapists in this piece came directly from therapists in the zynnyme community, used with their permission, with names changed for privacy. All other claims are sourced above.
Miranda Palmer, LMFT, and Kelly Higdon, LMFT, are the co-founders of zynnyme, a business education and coaching company for therapists in private practice. Twenty years in, they have coached tens of thousands of therapists out of exploitative arrangements with insurance companies and venture-backed platforms. They are co-authors ofTherapist Burnout andBeyond the Hour, and co-hosts of theStarting a Counseling Practice Success Stories podcast.
The Power and Control Wheel adapted in this piece is based on the original Power and Control Wheel developed by the Domestic Abuse Intervention Project, Duluth, MN. We honor the women whose testimony built it. The full attribution sits on the wheel itself.